Reconstruction (Warning: graphic images)
Thank you to all the brave patients who have allowed us to share their journey.

BEFORE: post Mohs

AFTER: Cervical facial rotation flap. Important pointers: the superior aspect of the flap should reach the zygoma (or slightly above the lateral canthus) to suspend the flap upwards. Maintain redundancy of lower eyelid skin to prevent ectropion.

BEFORE: post Mohs

AFTER: Cervical facial rotation flap

BEFORE, trauma
AFTER, paramedian forehead flap, nostril revision

BEFORE, trauma

AFTER, paramedian forehead flap, nostril revision

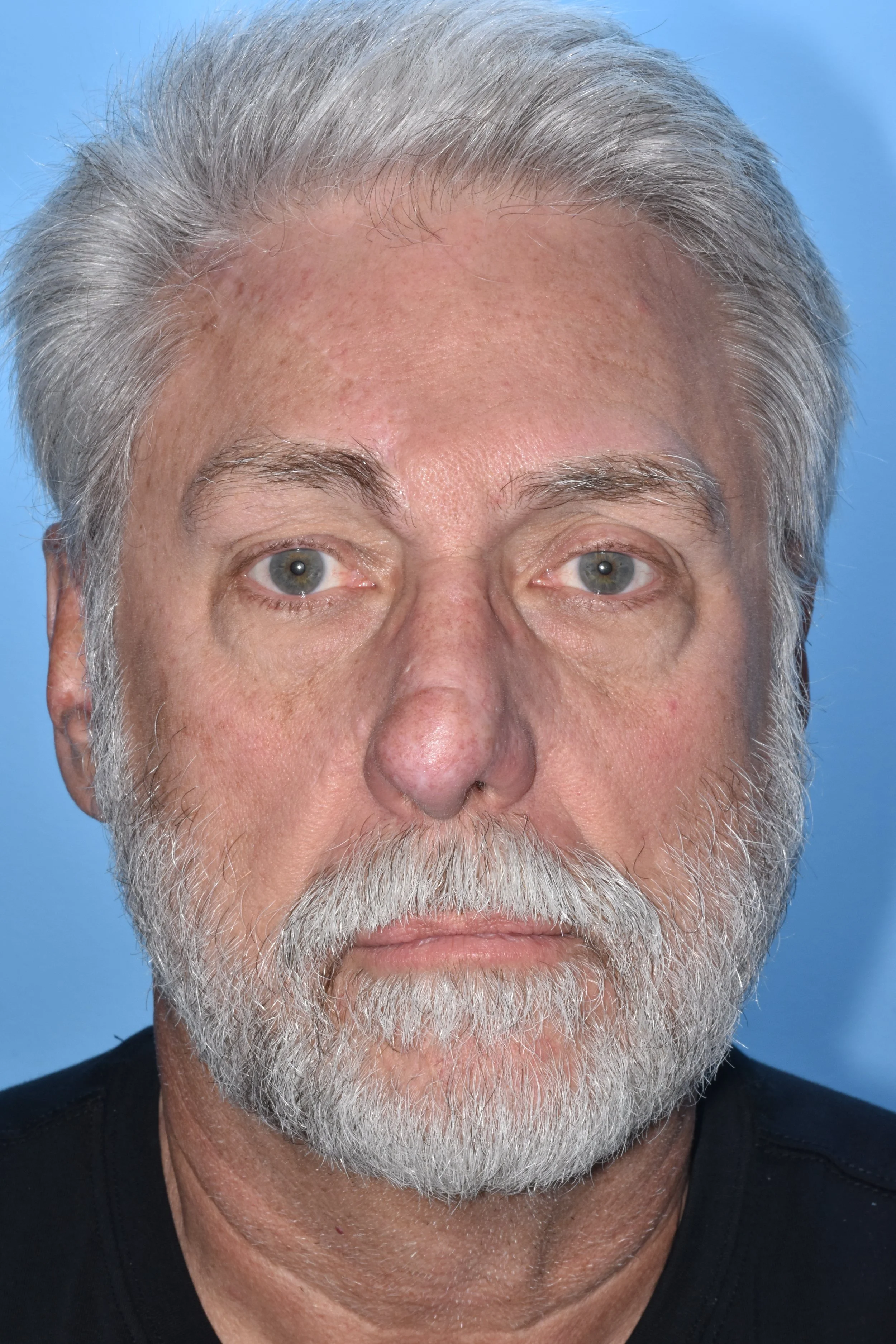
BEFORE, trauma

AFTER, paramedian forehead flap, nostril revision

Reconstruction of nasal defect with paramedian forehead flap, with additional nostril revision

BEFORE: partial amputation of helical rim after dog-bite injury

AFTER: rib reconstruction of ear, 2 stages.

BEFORE: Skin cancer prior to resection

BEFORE: completion of Mohs resection

AFTER: Paramedian forehead flap, defatting ala

AFTER: Paramedian forehead flap, defatting ala

AFTER: Paramedian forehead flap, defatting ala


BEFORE: Melanoma in situ

BEFORE: Melanoma in situ

BEFORE: Mohs resection for melanoma in situ

2w AFTER: Bipedicle advancement flap was advanced anteriorly from the preauricular region. Full-thickness skin graft was placed to cover the preauricular donor defect.

1y AFTER: Bipedicle advancement flap was advanced anteriorly from the preauricular region. Full-thickness skin graft was placed to cover the preauricular donor defect.

1y AFTER: Bipedicle advancement flap was advanced anteriorly from the preauricular region. Full-thickness skin graft was placed to cover the preauricular donor defect.